

ADVERTISEMENT
What You Should Know About Biofilms And Chronic Wounds
Biofilms reportedly cause an estimated 1 million nosocomial infections each year in the United States.1 Surgically, these microorganisms may cause abscesses, prosthetic failure and osteomyelitis. These complications may require surgical excision of the infected prosthesis and underlying soft tissue along with reconstruction of the affected part.
Understanding the nature of biofilms through research and clinical experience is key to providing the appropriate treatment. Moreover, such treatment and prevention may even lead to the eradication of serious, chronic illnesses and surgical complications.1
Biofilm may not be a familiar term but you have encountered it on a regular basis. The plaque that forms on teeth and causes decay is one type of biofilm. The “gunk” that clogs the drain is also biofilm. Biofilm forms when bacteria adhere to surfaces in moist environments by excreting a slimy, glue-like substance. Whenever you find a combination of moisture, nutrients and a surface, you are likely to find biofilms. Biofilms are held together by sugary molecular strands, collectively termed extracellular polymeric substances (EPS).
In order to understand the impact of chronic bacterial infection and host response, one must understand the nature of biofilms (see “A Closer Look At The Formation Of Biofilm” on page 50). These bacteria can be the source of various chronic diseases and increased mor- bidity. In surgical patients, they may cause latent infections that physicians see many weeks to months following a surgical procedure.1,2 Upon the initial treatment with antibiotics, the infection may respond. However, it may return at a later time despite a full course of antibiotic therapy. This is partly due to the natural composition of these bacteria, which allow them to develop drug resistance.1,2
Currently, there are no definitive methods for the diagnosis of a biofilm infection, except clinical suspicion and clinical presentation. Due to the lack of sound diagnostic technique, prevention of the infection is crucial.
Prophylactic prevention of biofilms is an important consideration for major podiatric surgical procedures. Advanced podiatric procedures, which require the use of prosthetic implants and biomaterials, such as stainless-steel pins used in external fixation frames, require judicious attention for the prevention of infection.These implants can be a source of biofilm infection. In fact, “pin tract infections in external fixation frames have been shown to occur in as much as 71 percent of patients.”1
Such complications often lead to osteomyelitis and possibly amputation of the affected part. Biofilm infection rates for orthopedic procedures, such as hip and knee replacements,“remain between 1 and 2 percent, and even higher for revisional surgical procedures.”1 These rates may or may not result from breaches in surgical aseptic technique.
Newer studies have indicated that treatment for these infections may involve local antibiotic therapy in addition to intravenous therapy. Current studies have also investigated natural treatments such as tea tree oil for biofilm infections involving the skin.1
Future treatment of biofilm infections may combine the use of prophylactic antibiotics and natural medications with surgical intervention.
What The Literature Reveals About Common Bacterial Biofilms
While some studies have isolated the most common microorganism (Staphylococcus epidermidis) that triggers biofilm infections, many other organisms have been isolated. Common bacteria found in biofilms include grampositive Enterococcus faecalis and Staphylococcus aureus. Gram-negative bacteria include Escherichia coli, Klebsiella pneumonia, Proteus mirabilis and Pseudomonas aeruginosa.1
Bacterial biofilms have a predilection for indwelling catheter devices and prosthetic grafts. A study by Bergamini, et al., noted that “Staphylococcus epidermidis was the most common isolated microorganism found in vascular prosthesis.”2 The study evaluated the efficacy of graft replacement as treatment for vascular prosthesis in a canine model. The researchers evaluated the established biofilm infection found on a prosthetic surface in the canines. In order to treat the infection, researchers utilized graft excision, parenteral antibiotics and graft replacement with a Dacron or polytetrafluoroethylene (PTFE) vascular prosthesis.2
After one month of graft replacement, the study authors found that “no PTFE graft had signs of infection” but approximately one-third exhibited “perigraft exudates and inflammation.” While the researchers suggested that graft replacement may improve healing, they noted that “colonization of the graft remained a considerable risk due to the resistance of the biofilm.”2
Shimabukuro, et al., examined local treatment of Dacron patch graft infected with S. epidermidis, utilizing antibiotic- releasing ceramic in a rat model.3 The study found “similar effectiveness against the Dacron patch graft infection with biofilm-producing S. epidermidis following local treatment with antibiotic- releasing ceramic for prosthetic graft infection.”3
Biofilm Microorganisms And Resistance: What You Should Know
In surgical patients, biofilms can lead to an increased morbidity and mortality.3 In podiatric procedures involving implants, these infections may cause limb-threatening complications. There is a rising demand for prophylactic antibiotic therapy in the prevention of biofilms for many podiatric surgical procedures.
Unfortunately, some systemic dosing levels of antibiotics, which were developed according to the pharmacodynamics and pharmacokinetics of planktonic organisms, are ineffective against biofilm microorganisms. Some researchers have noted that biofilm microorganisms are “100 to 1,000 times less susceptible to antibiotics than their planktonic counterparts.” They cite four main reasons for the resistance.Those reasons are:
• restricted penetration of the antibiotic through the biofilm;
• nutrient limitation, altered microenvironment and slow growth of biofilm cells;
• adaptive responses; and
• genetic alteration to “persister” cells.5
What The Studies Show About Biofilms And Antibiotic Treatment
In terms of specific antibiotic treatment, a study by LaPlante, et al., evaluated the effectiveness of daptomycin (Cubicin, Cubist Pharmaceuticals) and vancomycin on isolated biofilm strains.5 The study used daptomycin analytical powder, vancomycin analytical powder and heparin sodium.The test organisms were biofilmproducing reference strains of S. aureus and S. epidermidis, and a non-biofilm forming S. epidermidis as a control group.
The study authors determined that daptomycin concentrations of 1 mg/L inhibitied the development of S. epidermidis and S. aureus biofilm mass.5 They also found that vancomycin inhibited the formation of biofilm mass (S. aureus and S. epidermidis) at respective concentrations of 1 and 4 mg/L.5
Previous studies have also evaluated the efficacy of vancomycin and daptomycin in experimental foreign body infections and indwelling catheter devices.5
Vaudaux, et al., evaluated the activity of daptomycin and vancomycin in a rat model. They looked at subcutaneously implanted tissue cages infected with a clinical S. aureus isolate obtained from a patient with catheter-related sepsis.6 The study authors did not measure Staphylococcus aureus biofilm formation. After seven days of therapy with daptomycin or vancomycin, the researchers noted a “significant increase” in mean bacterial counts (CFU/mL) in comparison to implanted tissue cages of untreated animals. However, they noted no significant difference between the daptomycin and vancomycin groups.”6
Lee, et al., investigated several antimicrobial agents to determine an optimal concentration and duration for antibiotic lock solutions to effectively treat catheter-related infections caused by biofilm-producing S. epidermidis and S. aureus.7 They evaluated antimicrobial doses of 1, 5 and 10 mg/mL with dwell times of one to 14 days. The study demonstrated that “an antibiotic lock with vancomycin solution (5 mg/mL, changed every 48 hours) cleared S. epidermidis and S. aureus from the in vitro model after a five-day dwell time.”7
Another study by Giacometti, et al., investigated vancomycin in a staphylococcal central venous catheter infection in a rat model.8 They found that “MIC and MBC of vancomycin and other agents against the adherent bacteria were at least fourfold higher than those against freely growing cells.”8 They also determined “no significant reduction” of bacterial concentration within the catheter model system during this time.8
Addressing Biofilm Formation On Surgical Devices
Biofilm formation may result in serious complications following various surgical procedures. When using external fixation frames for limb reconstruction in podiatric surgery, surgeons often employ stainless steel wires. These implants may act as “foreign” objects to the body. In turn, bacterial organisms invade the foreign objects, stimulating the body’s immune response.
A study conducted by Van der Borden, et al., investigated the use of electric current for the detachment of Staphylococcus epidermidis biofilms from stainless steel.10 The researchers evaluated implants that are typically utilized in orthopedic and podiatric surgical procedures. The experiment used four separate currents (60 DC and block current and 100 DC and block current). The study authors applied each current for a total of 360 minutes to enhance detachment of the biofilm.They noted a higher percentage of biofilm detachment with DC currents.10
The Centers for Disease Control and Prevention (CDC) have called for increased research in key areas in order “to better understand and control biofilms on indwelling medical devices.”4 The CDC emphasized the importance of developing “more reliable techniques” for collecting and measuring biofilms.4 Specifically, the CDC maintains that while current quantification methods detect biofilms in catheter-related devices, these methods do not allow one to quantify the inner lumen surface of the catheter for biofilm contamination.4
In a study conducted by the CDC, Zufferey, et al., described a method for rapidly detecting biofilm cells on catheters via direct staining of the catheter with acridine orange.4 The study revealed that this quantification technique provided more rapid results than current standards without quantifying cells. They suggested that “techniques that allow counting of biofilm cells directly on the catheter surface would be an improvement over established methods.”4
Zufferey, et al., also concluded that “a greater understanding of cell-to-cell communication within biofilms may lead to better predictability of biofilm processes such as detachment as well as more effective control strategies.”4
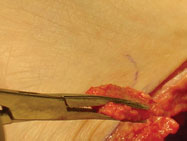
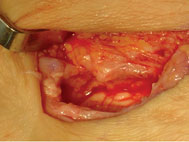
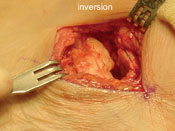
Case Study: When There Is Biofilm Formation On An Implant
A 54-year-old female farmer received a referral to our clinic by her previous surgeon. She had a history of a painful left flatfoot deformity associated with posterior tibial tendon dysfunction (PTTD).A subsequent surgery in February 2003 consisted of a subtalar joint arthroereisis (MBA) and posterior tibial tendon augmentation/ advancement. She demonstrated uneventful healing with a return to full farming activities.
In July 2004, without a history of preceding trauma, she demonstrated pain, edema, erythema and drainage over the lateral sinus tarsi incision.Vital signs were normal. The MRI demonstrated fluid collection in the sinus tarsi suspicious for residual abscess without evidence of talar or calcaneal osteomyelitis. Culture and sensitivity recovered Pseudomonas aeruginosa. She received appropriate IV antibiotics for six weeks and responded well.All symptoms subsided and she returned to full activities.
In August 2005, the patient again demonstrated pain, edema and erythema without drainage. She again received IV antibiotics for four weeks. All symptoms disappeared and she returned to farming activities.
The third episode occurred in February 2006 with an abrupt onset of pain, erythema, heat, fever and chills. Her surgeon referred her to our clinic. A Ceretec scan was positive for bone involvement in the sinus tarsi. After conducting an appropriate workup, we removed the MBA implant, debrided bone and soft tissue, and placed an arthroereisis device into the tarsal canal. The device was fabricated from vancomycin-impregnated polymethylmethacrylate (PMMA) beads.We also placed her on vancomycin for four weeks. The intention was to eventually perform a subtalar joint arthrodesis but the patient has remained asymptomatic for two years, and enjoys full activities.
This case history demonstrates the tenets of a biofilm.There was a surgical procedure with an implant that was asymptomatic for an extended period of time after her operation (17 months). She apparently responded well to IV antibiotics during two episodes of biofilm inflammatory resections over the next 19 months. Eventually, we removed the implant and performed aggressive debridement of osseous and soft tissue. In this classic case of biofilm infection, the patient has responded well.
In Summary
Although more research has been dedicated to understanding the nature of biofilms and disease, less is known about the best method for elimination. There is also a need for the development of diagnostic techniques in order to provide appropriate treatment. In addition to proper diagnostic techniques, research must be dedicated to proper collection and culturing of samples of these microorganisms for analysis.1
While most biofilm infections may resolve with antibiotic therapy, newer studies suggest that local antibiotic therapy may also reduce biofilm burden. In a surgical setting, prevention of these microorganisms involves the use of pro- phylactic intravenous antibiotics in addition to regular sterile dressing techniques.
Once more effective diagnostic techniques and treatment solutions emerge for bacterial biofilms, surgeons may be able to eliminate resulting surgical complications from biofilms. This could limit hospital stay and decrease overall healthcare costs.
Dr. Pupp is on the Residency Training Committee in the Department of Podiatric Medicine and Surgery at the Providence Hospital and Medical Center in Southfield, Mich. He is a Fellow of the American College of Foot and Ankle Surgeons. Dr.Williams is a PGY-II Resident at the aforementioned Providence Hospital and Medical Center.
References:
1. Nielson D, Pupp G. Biofilms and infection, what you should know. Podiatry Today 19(11):26-31, 2006.
2. Bergamini T, Bandyk D, Govostos D. Infection of vascular prostheses caused by bacterial biofilms. JVasc Surg 7: 21-30, 1998.
3. Shimabukuro K, Hirose H, Mori Y, Takagi,H. Local treatment of Dacron patch graft infected with biofilm-producing Staphylococcus epidermidis using antibioticreleasing porous apatite ceramic: an experimental study in the rabbit. J Vasc Surg 39:1361, 2004.
4. Zufferey J, Rime B, Francioli P, Bille J. Simple method for rapid diagnosis of catheter-associated infection by direct acridine orange staining of catheter tips. J Clin Microbiol 26:175-7, 1988.
5. Laplante K, Mermel L. In vitro activity of daptomycin and vancomycin lock solutions on staphylococcal biofilms in a central venous catheter model. Neprology and Transplantation, on-line publication, doi:10.1093/ndt/gfm141, 2007.
6 Vaudaux P, Francois P, Bisognano C, Li D, Lew DP, Schrenzel J. Comparative efficacy of daptomycin and vancomycin in the therapy of experimental foreign body infection due to Staphylococcus aureus. J Antimicrob Chemother 52:89–95, 2003.
7. Lee JY, Ko KS, Peck KR, Oh WS, Song JH. In vitro evaluation of the antibiotic lock technique (ALT) for the treatment of catheter-related infections caused by staphylococci. J Antimicrob Chemother 57:1110–1115, 2006.
8. Giacometti A, Cirioni O, Ghiselli R, et al. Comparative efficacies of quinupristin-dalfopristin, linezolid, vancomycin, and ciprofloxacin in treatment, using the antibiotic-lock technique, of experimental catheter-related infection due to Staphylococcus aureus. Antimicrob Agents Chemother 49:4042–4045, 2005.
9. Brady A, Loughlin R, Gilpin, D, et al. In vitro activity of tea-tree oil against clinical isolates of methicillin-resistant and sensitive Staphylococcus aureus and coagulase-negative staphylococci growing planktonically and as biofilms. J of Medical Microbiology 55: 1375- 1380, 2006.
10. Van der Borden A,Van der Werf H, et al. Electric–induced detachment of Staphylococcus epidermidis biofilms from surgical stainless steel. Applied and Environmental Microbiology 70: 6871-6874, 2004. Additional References
11. Stoodley P, Kathju S, Erdos G, Hu F, et al. Session II: Dealing with biofilms: molecular and imaging techniques for bacterial biofilms in joint arthroplasty infections. J of Clinical Orthopedics and Related Research 437: 31-40, 2005.
12. Bayston R, Ashraf W, Barker-Davies R, Tucker E, et al. Biofilm formation by propionibacterium acnes on biomaterials in vitro and in vivo: impact on diagnosis and treatment. J of Biomedical Materials Research; on-line publication, doi:10.1002/jbm.a.31145, 2006.
For related articles, see “Biofilms And Infection: What You Should Know” in the November 2006 issue of Podiatry Today or “Key Insights On Addressing Infected Hardware” in the August 2006 issue.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}