

ADVERTISEMENT
A Guide To Transmetatarsal Amputations In Patients With Diabetes
Lower extremity limb preservation among patients with diabetes continuously challenges the foot and ankle surgeon. With a significant population afflicted by this disease, podiatric physicians often perform amputations, a complication related to diabetes.1-4 The literature shows that pedal amputations occur in 60 percent of all nontraumatic lower extremity amputations with foot related disease as the most frequent cause for hospital admission.4,5 Transmetatarsal amputations, a common partial foot amputation, succeed with long-term effectiveness in limb salvage and function.1-3,6-19 Compared to more proximal pedal amputations, this midfoot procedure proves to be the best option in respect to healing, function, patient satisfaction and long-term results.1 Current literature often refers to the introduction of transmetatarsal amputations by Bernard and Heute in 1855.20 However, the initial application for trench foot has expanded. McKittrick later applied the procedure to other indications and introduced the adjunctive use of antibiotic therapy as a means toward facilitating a functional, salvaged limb.9 McKittrick emphasized antibiotic therapy as an integral treatment of transmetatarsal amputations for diabetic infections.9 Indications for a transmetatarsal amputation include forefoot ailments due to infection, neuropathy, ischemia and chronic ulcerations.3,6,8-10,12,14,16,22,23 Often, a combination of the aforementioned indications complicates the presentation.1 Due to a number of factors, conservative treatment often fails. In many instances, such as gangrene or chronic wounds, a transmetatarsal amputation remains the only viable option for pedal salvage. Ulcerations are not uncommon in patients with diabetes due to decreased neurovascularity and uncontrolled glucose. The continuous requirement for wound care is time-consuming, expensive and often futile due to the diminished vascularity clinicians often encounter. These chronic wounds may become worse and lead to osteomyelitis. When pathology is localized to the forefoot, removing necrotic osseous and soft tissue structures of the forefoot can provide a healing environment and a high probability of a functional limb.
Essential Keys To The Preoperative Evaluation
The healing and success of the transmetatarsal amputation depends on many factors. Podiatric physicians must assess for common comorbidities, such as coronary artery disease, hypertension, renal disease and tobacco use, as they can affect and exacerbate the diminished health status of the diabetic population.2,6,10,12,13,16,21 Among patients with diabetes, decreased immmunocompromised health status and noncompliance issues contribute to the pathological pedal condition. Ensuring a multispecialty approach — with the aid of an internist, cardiologist and infectious disease specialist — can perioperatively optimize a patient’s medical status. During the initial evaluation, podiatrists should review the neurovascularity, dermatology and musculoskeletal status of the lower extremity for healing potential. There must be adequate, viable soft tissues available for coverage of the amputation site upon completion of the debridement. One should also check to see if there is decreased vascular status proximal to the forefoot. Indeed, sufficient vascularity is paramount for the healing of a transmetatarsal amputation.15 Angiogenesis is an important factor during the process of wound healing. Ischemia and severe distal atherosclerosis, a frequent finding in patients with diabetes, contribute to the failure of limb salvage.2,3,5,10,15,17,24-27 Diminished pedal pulses and abnormal Doppler waveforms provide clinical evidence of vascular disease and indicate poor healing potential.28 Accordingly, noninvasive vascular studies are indicated to evaluate the severity of ischemia and the potential of revascularization. Ultrasonic Doppler pulse volume recordings (PVR), blood pressure measurements and transcutaneous oximetry (TcPO2) measurements may suggest positive predictive values for healing.2 Keep in mind that ankle pressures may be poor indicators for healing.28 Transcutaneous oximetry and pulse volume recordings at the midfoot level have shown reliability in predicting healing.10,11 More accurate pressure measurements may be reflected in digital pressures due to falsely elevated ankle pressure from noncompressible arteries and calcified vessels.2,3,6,7,22,29
Why You Might Consider Referring A Patient For Revascularization
When vascular studies produce suboptimal results, clinicians may want to consider a referral for revascularization. Standard angiography and magnetic resonance angiography provide more information and further evaluation of the vascularity. In addition, when surgical intervention is indicated, these modalities assist in surgical planning by providing the anatomical definition of the occlusive disease. Patients with diabetes and multiple comorbidities often undergo revascularization with either a surgical bypass or endovascular intervention including a percutanaeous transluminal angioplasty (PCTA) or stent placement.30 Revascularization significantly increases healing potential with promising limb salvage results.8,10,15,16,24,25,31-35 Revascularization typically precedes the transmetatarsal amputation for optimal healing. Expeditious revasculariation increases antibiotic therapy to the lower extremity to facilitate eradication of the infection.28 A delay in amputation permits soft tissue improvement due to an increase in soft tissue viability when the vascular supply normalizes.28 Researchers have emphasized the importance of revascularization followed by a subsequent amputation for a successful outcome.2,7,13,15,21 An ultrasound Doppler allows the evaluation of the vessel patency. In emergent cases, such as wet gangrene, detailed vascular evaluation is not possible and one should undertake it after the transmetatarsal amputation.
How Neuropathy And Equinus Affect The Preoperative Picture
Neuropathy, particularly distal symmetric polyneuropathy, affects more than 50 percent of the diabetic population.36 Decreased neurological status also contributes to ulcerations and amputations.1 In order to detect sensory loss during a physical examination, one may evaluate protective sensation with a 5.07 Semmes-Weinstein 10-g nylon filament. The evaluation of vibration with a 128-Hz tuning fork and proprioception are also pertinent in the neurological examination.1,36,37 While sensory neuropathic symptoms consist of pain, paresthesia, numbness and loss of protective sensation, motor neuropathy correlates with muscular atrophy, motor imbalance and related pedal deformities. Flexor, extensor and intrinsic musculature imbalance lead to digital deformities. The deformities at the digits produce retrograde pressure onto the metatarsals, further altering gait and pressures.1 Ulcerations form from the abnormal pressure distribution and often wounds present plantar to the metatarsal heads.1 Insufficient neurovascularity correlates to the atrophic, fragile skin of the patient with diabetes. A dermatological evaluation reveals shiny, scaly skin, which indicates decreased vascularity. One should also examine chronic neuropathic wounds for signs of infection and the possibility of osteomyelitis. Preoperative planning for the excision of necrotic tissue and wounds is imperative to ensure an adequate soft tissue envelope will exist with the amputation of the forefoot. Although podiatric surgeons commonly use plantar skin flaps after performing these procedures, one should investigate other options if plantar skin flaps are not possible. In the biomechanical examination, one must assess range of motion, strength, ambulation and deformities of the lower extremity. Ankle equinus and varus deformities are not uncommon.1 Glycosylation and contracture of the Achilles tendon with a subsequent equinus deformity pose another difficulty within the diabetic population.25,32,34 Dorsiflexion of the ankle at 10 degrees with the knee extended and 15 degrees with the knee bent is required during the gait cycle. Recurrent ulceration and abnormal pressure at the forefoot due to an equinus contracture correlate to a limited range of motion at the ankle and decreased strength of the Achilles tendon. An equinus deformity makes preexisting deformities worse and alters the biomechanics of gait. In correcting or preventing equinus, an Achilles tendon lengthening procedure may be required in conjunction with a partial foot amputation.24 Nishimoto, et. al., described the importance, indications, techniques and pitfalls of Achilles tendon lengthening.32 While the Achilles tendon may be modified, preserving other tendons, specifically the tibialis anterior and peroneus brevis tendons, prevents further post-op contractures by allowing inversion and eversion respectively. Scarring of the extensor tendons contributes to ankle dorsiflexion and resists the equinus force of the anterior tibialis tendon.11,28 One may apply a split tibialis anterior tendon transfer for a varus deformity.6 Laboratory values, an integral portion of patient treatment, include a complete blood count with differentials, Chemistry-7 and coagulation parameters. Wound healing parameters consist of glucose levels, hemoglobin, lymphocytes, glycosylated hemoglobin (HgA1C) and albumin. Glycosylated hemoglobin more accurately reflects the overall diabetic management of blood glucose control. Albumin and total lymphocyte counts validate the nutritional status and the capacity to resist infection.1,6,22,38 White blood cell count, erythrocyte sedimentation rate and c-reactive protein may indicate infection.
When An Emergent Amputation Is Required
The definitive treatment for wet gangrene is immediate aggressive surgical debridement of the offending tissues and antibiotic therapy.6,11,39 Wet gangrene, caused by bacterial infection in a dysvascular and anoxic environment, rapidly disseminates and may cause death if not treated properly.40 A transmetatarsal amputation allows the elimination of virulent invasive local infection and prevention of septicemia.9 Often one would perform a guillotine amputation to remove all necrotic soft tissue and bone.11 The surgical wound remains packed open to allow the stabilization of the foot. With the eradication of the infection and a stable foot, one may evaluate skin closure and revascularization.11 Due to the emergent situation of the requirement and lack of time, one should evaluate revascularization postoperatively.
Key Insights On Performing Transmetatarsal Amputations
The surgeon must not dismiss important principles of surgery such as gentle tissue handling, hemostasis and meticulous anatomical dissection. Viable plantar soft tissues and adequate resection of osseous structures for closure are paramount. Due to decreased vascularity, one should not use a tourniquet. Tourniquets prevent the proper assessment of bleeding and damage distal bypass sites.6,28 An ankle block should be sufficient for anesthesia.28 Small towel clamps at preaxial and postaxial phalanges assist in the control of the forefoot during the dissection. The surgeon should make a full thickness dorsal incision proximal to the metatarsophalangeal joints and necrotic tissue, and continue plantarly in order to ensure an adequate plantar flap. A larger medial flap side accommodates the increased medial forefoot diameter. One should proceed to dissect the dorsal soft tissue plane from the metatarsals and follow this with disarticulation of the metatarsophalangeal joints. The transverse sectioning and beveling of the metatarsals proximal to the surgical neck in the functional metatarsal parabola optimizes the weightbearing surfaces.6 Bevel the metatarsals plantarly, with the first and fifth beveled at the medial and lateral aspects respectively.6 Within the parabola, the second metatarsal is the longest, followed by the first, the third, fourth and fifth. An oblique metatarsal break and graded step down pattern allow propulsion and preserve the gait pattern. The lack of existing osseous prominences prevents high-risk pressure areas. Remodeling the osseous resection may be necessary to remove necrotic tissues. In addition, more osseous resection increases the availability of soft tissue coverage. Prior to closure, one should reevaluate the excision of superfluous soft tissue and osseous structures. Sesamoid bones, plantar plates, nerves and tendons serve as a nidus for infection. With distal retraction of extensor and flexor tendons, one can resect tendons proximally to allow retraction.6 Resecting nerves proximally helps avoid a neuroma or neuritis on any osseous prominences.6 Employing a system that provides pulsatile irrigation and debridement can facilitate copious lavage of the surgical wound. Electrocautery prevents excessive bleeding and the formation of a hematoma.
Pertinent Pearls For Ensuring Successful Wound Closure
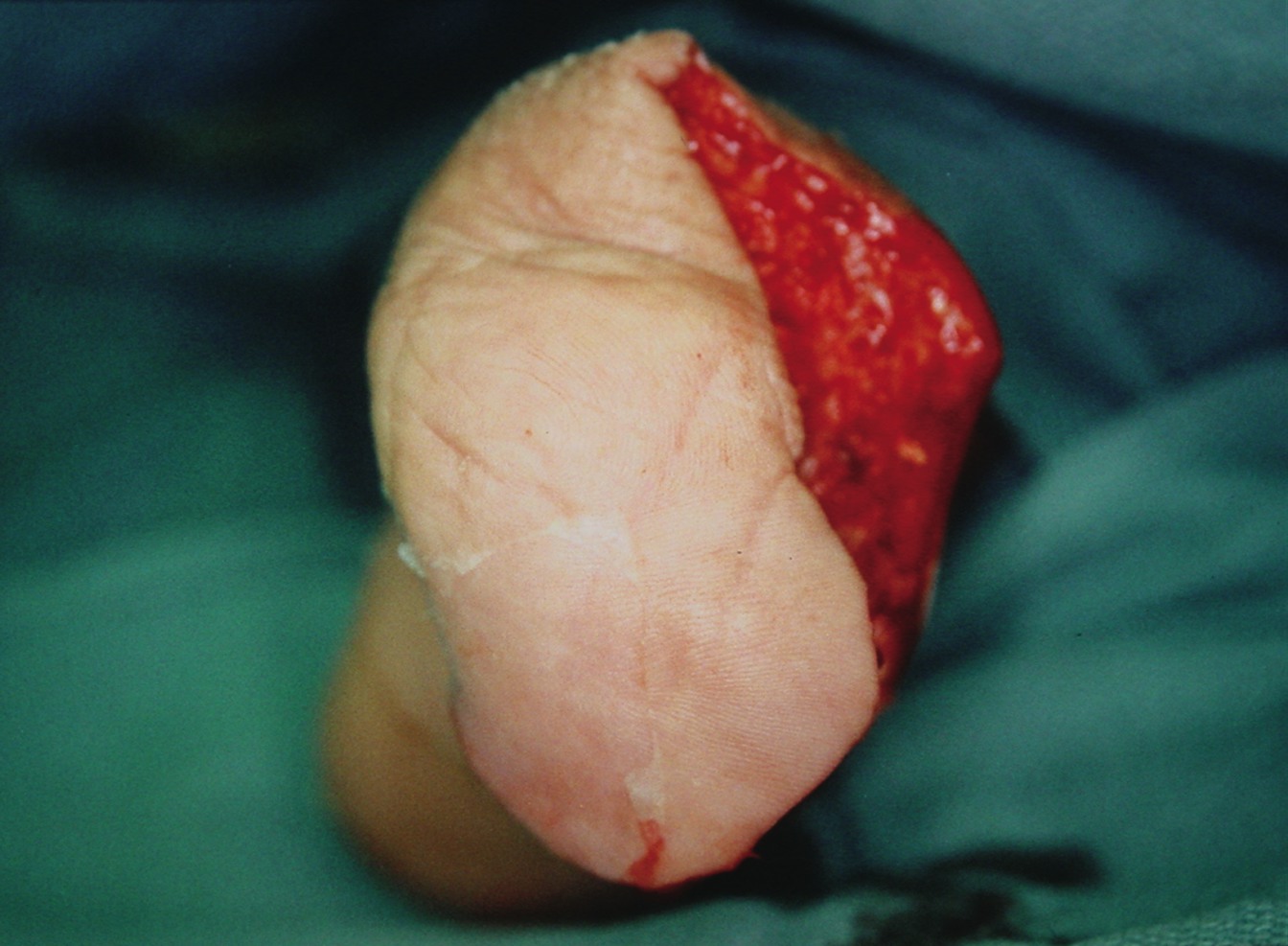
Primary closure by the plantar flap is ideal due to the vast arterial supply from the plantar artery.8,41 After revising the dermal thickness and skin edges, performing a dorsal approximation of the plantar skin flap allows closure. Surgical wound closure consists of nonabsorbable simple interrupted sutures. Deep sutures are not required due to the possible of dysvascularity. It is imperative to ensure approximation without skin tension, adequate capillary fill time and vascular skin presentation in order to prevent dehiscence and ischemia. Apply a sterile, bulky, protective dressing with adequate compression and the use of abdominal padding. Avoid using a constrictive dressing.28 If a plantar flap is not available due to nonviable skin, the surgeon should explore other options for closure.6,10,11,28 One may use a combination of flaps, grafts and soft tissue modification and mobilization, depending on the available cutaneous tissue after functional soft tissue and osseous contouring. Local flaps and the transposition of neighboring vascularized soft tissue allow coverage of a large defect. Flaps contain viable skin without the presence of local necrosis and infection.38 In addition, flaps with extrinsic and intrinsic vascularity improve vascularity. Limitations of flaps are closure of the donor area and the vascular pedicle, which determines the rotational arc. The split thickness skin graft, which is often acquired from the anterior thigh of the ipsilateral leg, requires a healthy granular recipient site. Meshing allows coverage of a larger area and decreases complications such as a seroma or hematoma. For the protection and viability of the skin graft, a bolster dressing augments the graft with sutures minimizing sloughing and securing the wound tissues. Delayed primary closure and secondary healing are also options. Delayed primary closure, which one would perform three to five days after the amputation, facilitates closure for procedures secondary to sepsis with the eradication of the infection and a stable limb. Negative pressure wound therapy accelerates healing by secondary intention. The application of subatmospheric pressure protects the wound while promoting perfusion and a moist healing environment. In one study, an open transmetatarsal amputation proceeded to a more proximal amputation compared to those closed primarily.8 Accordingly, one should attempt every effort to facilitate primary closure. With numerous options for soft tissue coverage, one can achieve the ultimate goals of propulsion, function and healing.
Postoperative Management: What You Should Know
Proper postoperative management is essential for transmetatarsal amputations. If the amputation is subsequent to an infection, one should continue antibiotic therapy. Wound care and offloading the foot are paramount to healing of the surgical area. One should use a protective, compressive dressing until there is biological epidermal closure. The patient has achieved this closure and healing when there is complete integrity to the epidermal and dermal layers. Sutures remain for approximately three to six weeks. Wound dehiscense and ulceration are the most common complications leading to failure of the amputation.16 Failure to heal occurs in a significant population due to decreased vascularity, increased pressure, hyperglycemia and infection.2,10,11,14,15,23,42 Poor results due to severe vascular disease may occur if one did not address this condition preoperatively.15 Noncompliance in regard to maintaining nonweightbearing status and ignorance to abnormal pressures at the stump result in ulcerations. An unhealed surgical wound, dehiscence and ulcerations inhibit function due to instability and abnormal pressure distribution. One should continuously emphasize the importance of nonweightbearing to the patient. Hyperglycemia inhibits critical components of the wound healing process and new capillary growth central to the wound healing process.43 Fibroblasts, connective tissue cells which secrete extracellular matrix rich in collagen, become dysfunctional with inadequate glucose levels. This leads to an impairment of collagen deposition. Infection and the risk of a deep vein thrombosis are also complications. Inadequate resection of necrotic, infected tissues and the failure of proper antibiotic usage may lead to infection. An infectious disease physician plays an integral role in the efficacy and long-term treatment of antibiotic therapy. With consultation of an internist or the patient’s primary care physician, coagulation therapy decreases the risk of thrombosis. Unfortunately, noncompliance is a major problem for patients with diabetes. Ensuring proper surgical patient selection contributes to a successful outcome.15 It is also important to emphasize patient education and their understanding of possible complications. Once the wound has adequately healed, the patient commences gait training. Physical therapy and prosthetics are useful for attaining and maintaining a functional stump. Physical therapy assists with limb function through gait training with assistive ambulation devices. Independent walking with the use of an ambulatory assistive device, shoe modifications, shoe filler or orthoses qualifies as successful ambulation. A healed stump does not require a prosthesis, which allows better function.18 Physical therapy integrates strength and range of motion exercises to prevent an equinus deformity. A prosthetist can provide proper shoegear, shoe modifications and fillers to neutralize pressure at the stump.
In Conclusion
Transmetatarsal amputations for ischemic and infected lower extremities persist as a viable option for limb salvage and function. This procedure eliminates a diseased, functionless extremity and restores function and ambulation.7,44 Preserving the rearfoot and midfoot decreases the overall energy required during function with a more proximal amputation.1,3,23,27,38,45 Accordingly, partial pedal amputations provide an alternative to the increased energy expenditure and the 65 percent increase in oxygen consumption during ambulation in leg amputees.44,46 Reduced energy expenditure during function, preservation of a more normalized gait, and the promising outlook with the use of prosthetic aids support this partial pedal amputation. An aggressive limb salvage approach can deter further proximal amputation and increase the quality and length of life. When considering this procedure among patients with diabetes, one should ensure a thorough preoperative evaluation. One should always evaluate a patient with diabetes for this procedure. Decreased vascularity and immunocompromised status should not deter the chance of a patient having a transmetatarsal amputation. While the possibility of a more proximal amputation cannot be predicted, one should pursue aggressive limb salvage when possible. The success of a transmetatarsal amputation can depend on multifactorial issues such as revascularization, wound healing factors and demographics. Unfortunately, exact healing factors remain unknown. An aggressive approach to amputations and revascularization is imperative for lower extremity salvage. Transmetatarsal amputations continue to restore lower limb function and improve the lifestyle of patients with diabetes. Dr. Salonga is a second-year resident at the Yale-New Haven Podiatric Surgical Residency Program in New Haven, Ct. Dr. Blume is an Assistant Clinical Professor of Surgery in the Department of Orthopaedics and Rehabilitation at the Yale University School of Medicine. He is Director of Limb Preservation at Yale New Haven Hospital in New Haven, Conn. Dr. Blume is a Fellow of the American College of Foot and Ankle Surgeons. References 1. Sanders LJ, Dunlap G. Transmetatarsal amputation: a successful approach to limb salvage. J Am Podiatr Med Assoc 82(3):129-135, 1992. 2. Stone PA, Back MR, Armstrong PA, et. al. Midfoot Amputations Expand Limb Salvage Rates for Diabetic Foot Infections. Ann Vasc Surg 19(6):805-11, 2005. 3. Hosch J, Quiroga C, Bosma J, Peters EJG, Armstrong DG, Lavery LA. Outcomes of transmetatarsal amputations in patients with diabetes mellitus. J Foot Ankle Surg 36(6):430-434, 1997. 4. Center for Disease Control and Prevention. National Diabetes Fact Sheet: General Information and National Estimates on Diabetes in the United States, 2005. Atlanta, Ga:U.S. Department of Health and Human Services, Centeres for Disease Control and Prevention, 2005. 5. Williams DT, Harding KG, Price P. An Evaluation of the Efficacy of Methods Used in Screening for Lower-Limb Arterial Disease in Diabetes. Diabetes Care 28:2206-10, 2005. 6. Funk C, Young G. Subtotal Pedal Amputations: Biomechanical and Intraoperative Considerations. J Am Podiatr Med Assoc 91(1):6-12, 2001. 7. Mwipatayi BP, Naidoo NG, Jeffrey PC, Maraspini CD, Adams MZ, Cloete N. World J Surg 29(2):245-8, 2005. 8. Toursakissan B, Hagino RT, Khan K, Schoolfield J, Shireman PK, Harkless L. Healing of Transmetatarsal Amputation in the Diabetic Patient: Is Angiography Predictive? Ann Vasc Surg 19(6):769-73, 2005. 9. McKittrick LS. Recent advances in the care of the surgical complications of diabetes mellitus. N Engl J Med 235:929-932, 1946. 10. Miller N, Dardik H, Wolodiger F, Pecoraro J, Kahn M, Ibrahim IM, Sussman B. Transmetatarsal amputation: The role of adjunctive revascularization. J Vasc Surg 13(5):705-711, 1991. 11. Durham JR, McCoy DM, Sawchuk AP, et al. Open transmetatarsal amputation in the treatment of severe foot infections. Am J Surg 158(2):127-130, 1989. 12. Thomas SR, Perkins JM, Magee TR, Galland RB. Transmetatarsal Amputations: An 8 Year Experience. Ann R Coll Surg Engl. 88(3):164-6, 2001. 13. Sheahan MG, Hamdan AD, Veraldi JR, et. al. Lower Extremity Minor Amputation: The Role of Diabetes Mellitus and Timing of Revascularization. J Vasc Surg 42(3):476-80, 2005. 14. Hobson M, Stonebridge PA, Clason A. Place of transmetatarsal amputations: a 5-year experience and review of the literature. J R Coll Surg Edinb 35(2):113, 1990. 15. La Fontaine J, Reyzelman A, Rothenberg G, Husain K, Harkless LB. The role of revascularization in transmetatarsal amputations. J Am Podiatr Med Assoc 91(10):533-535, 2001. 16. Pollard J, Hamilton G, Rush S, Ford L. Mortality and Morbidity After Transmetatarsal Amputation: Retrospective Review of 101 Cases. JFAS 45(2):91-97, 2006. 17. Crinnon J, Hicks D. Transmetatarsal Amputation: an 8 Year Experience. Ann R Coll Surg Engl 83, 2001. 18. Geroulakos G, May AR. Transmetatarsal Amputation in Patients with Peripheral Vascular Disease. Eur J Vasc Surg 5, 1991. 19. Ohsawa S, Inamori Y, Fukuda K, Hirotuji M. Lower Limb Amputation for Diabetic Foot. Arch Orthop Trauma Surg 121, 2001. 20. Bernard C, Huete C, quoted by Schwindt CD, Lulloff RS, Rogers SC. Transmetatarsal amputations. Orthop Clin North Am 4:31-42, 1973. 21. Glass H, Rowe VL, Hood DB, Yellin AE, Weaver FA. Influence of Transmetatarsal Amputation in Patients Requiring Lower Extremity Distal Revascularization, Am Surg 70(10):845-9, 2004. 22. Wallace GF, Stapleton J. Transmetatarsal Amputations. Clin Pod Med Surg. 22,2005. 23. Schwindt CD, Lulloff RS, Rogers SC. Transmetatarsal Amputations. Orthop Clin N Am:4(1), 1973. 24. Pomposelli FB, Marcaccio EJ, Gibbons GW, Campbell DR, Freeman DV, Burgess AM, Miller A, LoGerfo FW. Dorsalis pedis arterial bypass: Durable limb salvage for foot ischemia in patients with diabetes mellitus. J Vasc Surg 21(3):375-384, 1995. 25. Reichle FA, Rankin KP, Tyson RR, Finestone AJ, Shuman CR. Long-term results of femoroinfrapopliteal bypass in diabetic patients with severe ischemia of the lower extremity. Am J Surg 137(5):653-656, 1979. 26. Roach JJ, Deutsch A, McFarlane DS. Resurrection of the amputations of Lisfranc and Chopart for diabetic gangrene. Arch Surg 122(8):931, 1987. 27. Chang BB, Bock DEM, Jacobs RL, et. al. Increased limb salvage by the use of unconventional foot amputations. J Vasc Surg 19(2):341-349, 1994. 28. Chang BB, Jacobs RL, Darling RC, Leahter RP, Shah DM. Foot Amputations. Surg Clin N Am 75(4), 1995. 29. Castaneda-Zuniga WR, Interventional Radiology 2nd ed, 1992. 30. DeSantis JT. Percutaneous Interventions for Lower Extremity Peripheral Vascular Disease. Am Fam Phys 64(12):1965-74, 2001. 31. Warren R, Crawford ES, Hardy IB, et. al. The transmetatarsal amputation in arterial deficiency of the lower extremity. Surgery 31:132, 1952. 32. Larsson J, Apelqvist J, Castenfors J, Agardh C, Stenstrom A. Distal blood pressure as a predictor for the level of amputation in diabetic patients with foot ulcer. Ft Ankle 14(5):247-253, 1993. 33. Santi MD, Thoma BJ, Chambers RB. Survivorship of healed partial foot amputations in dysvascular patients. Clin Orthop Rel Res 292:245-249, 1993. 34. Shah DM, Chang BB, Fitxgerald KM, Kaufman JL, Leather RP. Durability of the tibial artery bypass in diabetic patients. Am J Surg 156(2):133-135, 1988. 35. Rosenblatt MS, Quist WC, Sidawy AN, Paniszyn CC, LoGerfo FW. Results of vein graft reconstruction of the lower extremity in diabetic and nondiabetic patients. Surg Gyn Obstr 171(4):331-335, 1990. 36. Reamy BV. Preventing the Progression of Diabetes Mellitus. Am Fam Phys 71(3):425-8, 2005. 37. Meijer JW, Van Sonderen E, Blaauwwiekel et al. Diabetic Neuropathy Examination: A Hierarchy Scoring System to Diagnose Distal Polyneuropathy in Diabetes. Diabetes Care 23(6):750-3, 2000. 38. Pinzur M, Kaminsky M, Sage R, Cronin R, Osterman H. Amputations at the Middle Level of the Foot. JBJS 58-A(7),1986. 39. Griffith HW, Complete Guide to Symptoms, Illness and Surgery. Putnam Berkley Group, 1995. 40. Porth CM, Pathophysiology: Concepts of Altered Health. Lippincott, 1998. 41. Hidalgo DA, Shaw WW. Anatomic Basis of Plantar Flap Design. Plast Reconstr Surg 78(5):627-36, 1986. 42. McMurry JF. Wound healing with Diabetes Mellitus. Better Glucose Control for better wound healing in Diabetes. Surg Clin North Am 64(4):769-78, 1984. 43. Marston WA, Risk Factors Associated with Healing Chronic Diabeteic Foot Ulcers: the Importance of Hyperglycemia. Ostomy/Wound Manage 52(3):26-39, 2006. 44. McCollough NC. Orthopaedic Research in Amputation Surgery, Prosthetics and Orthotics. Prosthet Orthot Int 5(1):7-10,1981. 45. Garbalosa J. Foot Function in Diabetic Patients After Partial Amputation. Foot Ankle Int 17:43,1996. 46. Gonzalez EG, Corcoran PJ, Reyes RL. Energy Expenditure in Below-Knee Amputees: Correlation with Stump Length. Arch Phys Med Rehab 55(3):111-9, 1974.
References:
**sub**CE Exam #143**endsub** Choose the single best response to each question listed below. 1) Which of the following statements is true about the transmetatarsal amputation? a) It is contraindicated in the presence of gangrene. b) It is contraindicated in cases of infection. c) It may be the only viable option for pedal salvage in many instances such as gangrene and chronic wounds. d) None of the above 2) Diminished pedal pulses and abnormal Doppler waveforms … a) indicate vascular disease and poor healing potential. b) indicate vascular disease and moderate healing potential. c) may lead to the use of noninvasive vascular studies in order to evaluate the severity of ischemia and the potential of revascularization. d) a and c 3) _____significantly increases the healing potential of transmetatarsal amputations with promising limb salvage results. a) Offloading b) Revascularization c) Three to six weeks of adjunctive antibiotics d) None of the above 4) Neuropathy, particularly distal symmetric polyneuropathy, affects more than ____ percent of people with diabetes. a) 50 b) 30 c) 40 d) 75 5) During a dermatological exam of patients with diabetes, which of the following presentations indicates poor vascularity? a) Dull, scaly skin color with decreased turgor b) Shiny, atrophic skin c) Shiny, scaly skin with decreased texture and increased turgor d) None of the above 6) When it comes to the transmetatarsal amputation procedure, transverse sectioning and beveling of the metatarsals proximal to the surgical neck in the functional metatarsal parabola … a) optimizes the weightbearing surfaces. b) is contraindicated when one uses split thickness skin grafts. c) can help prevent a neuroma or neuritis on any osseous prominences. d) None of the above 7) Which of the following statements is true about flaps? a) They are indicated in the presence of local necrosis. b) Flaps improve vascularity. c) They are indicated in cases of infection. d) a and c 8) Which of the following statements is false about the split thickness skin graft? a) Using it in combination with a bolster dressing facilitates protection and viability of the graft. b) It requires a healthy granular recipient site. c) Meshing allows coverage of a larger area and decreases complications such as a seroma or hematoma. d) None of the above 9) In regard to delayed primary closure of a transmetatarsal amputation … a) the surgeon would perform this closure a week after the amputation. b) it is contraindicated for closure or procedures secondary to sepsis. c) the surgeon would perform this closure three to five days after the amputation. d) it is the ideal option due to the vast arterial supply from the plantar artery. 10) _____ and ____ are the most common complications leading to failure of the transmetatarsal amputation. a) Poor vascularity and dehiscent wounds b) Ischemia and ulceration c) Wound dehiscence and ulceration d) Hyperglycemia and ischemia Instructions for Submitting Exams Fill out the enclosed card that appears on the following page or fax the form to the NACCME at (610) 560-0502. Within 60 days, you will be advised that you have passed or failed the exam. A score of 70 percent or above will comprise a passing grade. A certificate will be awarded to participants who successfully complete the exam. Responses will be accepted up to 12 months from the publication date.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}