

ADVERTISEMENT
Exploring Limb Salvage Options In Patients With Chronic Limb Ischemia
Chronic critical limb ischemia has been defined as a non-healing ulceration or gangrene of the foot or toes, and/or rest pain that requires regular use of analgesics.1 These patients will require some type of intervention to resolve their condition. It can be particularly challenging to salvage the limb of a patient who has failed a bypass. The objective of revascularization is to augment blood flow to allow for wound healing and avoid major amputation resulting in the need for a prosthesis. Amputation of one or more digits or even transmetatarsal amputation preserves enough of the foot to allow for ambulation. However, after excision of the gangrenous segment, the surgical wound will not heal if there is inadequate blood flow to the area. Diabetic patients and others with limb-threatening ischemia often have few choices. Bypass surgery may not be possible due to poor vein quality or previous harvesting of saphenous veins for coronary artery bypass. Angioplasty for infrapopliteal vascular occlusive disease is not new. Dotter and Judkins described three patients with peroneal-tibial trunk angioplasty in their initial report in 1964.2 At first, coronary balloons were utilized and then specialized angioplasty balloons designed for tibial vessels became available.3 Limb salvage rates were similar to surgery. However, only 20 to 30 percent of patients with isolated tibial disease were candidates for endovascular therapy due to the number and length of lesions. Recently, Bolia, Brennan and Bell described subintimal angioplasty.4 Others have supported the role of this technique for limb salvage and have successfully treated longer lesions with close to 90 percent technical success.1,5 The development of cryoplasty therapy has advanced the mechanical properties of the angioplasty balloon, potentially transforming it into an instrument that alters the physiology of the plaque and smooth muscle cells. One uses liquid nitrous oxide to inflate the balloon for 20 seconds at 8 ATM. This cools the balloon to –10º C. The thinking is that this freezing action alters the plaque response to angioplasty, causing it to fracture more uniformly and reduce the incidence of flow-limiting dissections. There is a reduction in vessel wall recoil. Finally, the freezing action has been shown in vitro to activate markers of apoptosis. TUNEL assay and Annexin V assay revealed an apoptotic peak at –10º C and no apoptosis above 15º C. In theory, this suspends the ability of smooth muscle cells to secrete matrix, the basis of the restenotic lesion. With this in mind, let us consider a case study in which cyroplasty therapy was utilized in a combination approach to salvage the limb of a patient with chronic limb ischemia.
Case Study: A Patient With PVD And Chronic Limb Ischemia
The patient is a 72-year-old woman who was transferred from a local hospital for continued workup of her peripheral vascular disease (PVD) and ischemia of the third digit on the left foot. The patient had undergone an attempted left lower extremity bypass. However, the surgeons found the autogenous veins were unsuitable to serve as a conduit and the procedure was aborted. She was admitted to Yale-New Haven Hospital under the podiatric surgical service for a final attempt at limb salvage. The patient had a significant past medical history including PVD, diabetes, coronary artery disease, hypertension, hypercholesterolemia, myocardial infarction, chronic renal insufficiency, peripheral neuropathy and gangrene of the left third toe. She underwent a coronary artery bypass and cholecystectomy on Sept. 7. An attempted lower extremity bypass graft was unsuccessful on Sept. 24. Her medications included oxycodone hydrochloride 40 mg bid, atorvastatin calcium 10 mg daily, metoprolol 50 mg bid, amlodipine 5 mg daily, lisinopril 20 mg daily, stool softener 100 mg daily, aspirin 81 mg daily, a daily multivitamin and silver sulfadiazine cream. The patient is allergic to ibuprofen. In general, the patient was in no apparent distress and was alert and oriented. She had a regular heart rate and rhythm with positive S1 and S2 heart sounds. Her lungs were clear to auscultation bilaterally with no rhonchi, rales or wheezing. Her abdomen was soft, nontender and nondistended with positive bowel sounds. The lower extremity examination revealed a left, dry necrotic third digit with no discharge and no erythema. The patient had been using silver sulfadizaine cream on the dorsal and plantar aspects of the foot. The patient had nonpalpable dorsalis pedis and posterior tibial pulses with weak monophasic Doppler signals. Multiple ischemic lesions on the dorsal and plantar aspect of the forefoot were secondary to recent skin biopsies. The patient also had skin staples to the dorsum of the ankle and lower leg from the recent lower extremity bypass attempt.
What Did The Angiogram Reveal?
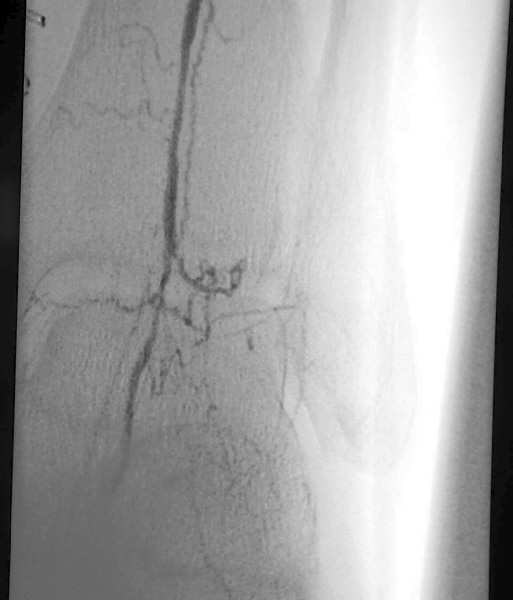
An angiogram revealed extensive tibial peroneal disease on the left limb with occlusion of all vessels to the mid-calf level. There was reconstitution in the anterior tibial that provided dominant flow to the foot and reconstitution of the dorsalis pedis artery. A MRI of the left foot revealed multiple areas of small abscesses associated with the ischemic ulcers but no evidence of osteomyelitis. After the failed bypass, vascular surgeons were consulted and repeat vein mapping confirmed the absence of a usable vein conduit. With the history of aborted left lower extremity bypass, the multidisciplinary team planned for endovascular limb salvage with interventional radiology. Noninvasive vascular testing included TcPO2 of the left pretibial region (49 mmHg) and the left dorsum (30 mmHg). A diagnostic angiogram prior to the aborted surgical procedure revealed a patent abdominal aorta, iliac arteries and left superficial femoral artery. The femoral bifurcation was intact. The above- and below-the-knee popliteal artery also was patent and without stenosis. The posterior tibial artery was occluded at the level of the mid-calf. The peroneal artery was severely diseased. The anterior tibial artery had proximal, hemodynamically significant stenosis and a 30 mm long occluded segment at the level of the lower one-third of the calf. There was hemodynamically significant stenosis of the dorsalis pedis artery at and just below the level of the ankle joint.
A Guide To Understanding The Cryoplasty Procedure
After completing angiogram procedures, surgeons performed an antegrade puncture of the left common femoral artery and placed a 6-Fr sidearm sheath with its tip in the proximal superficial femoral artery. A repeat diagnostic study confirmed the previous findings. The team subsequently used a 4-Fr Berenstein catheter with glide coating (Boston Scientific) loaded with a .014-inch guidewire (Sparta/Core 14, Guidant Corp.) to catheterize the anterior tibial artery and cross the stenosis. The vascular surgeons performed cryoplasty therapy with a 3 mm by 20 mm PolarCath Peripheral System balloon (CryoVascular Systems, Inc.). A post-op control angiogram showed excellent results with a less than 10 percent residual stenosis and no angiographic evidence of dissection. The vascular surgeons proceeded to turn their attention toward the occluded segment of the anterior tibial artery. They advanced the 4-Fr glide Berenstein catheter across the aforementioned treated segment and placed the tip of the catheter just above the occluded portion of the artery. After injecting contrast, the surgeons documented reconstitution of the post-obstructed anterior tibial artery. The surgical team crossed the obstructed segment with a 0.035-inch straight, stiff Glidewire (Boston Scientific), advanced the catheter across the obstruction and confirmed its intraluminal position with a contrast injection. Using the 3.0 mm balloon, they treated the obstructed segment with cryoplasty therapy. A post-op control angiogram disclosed minimal residual stenosis and no vessel wall dissection. There was no evidence of distal embolization of plaque fragments. The vascular surgeons advanced the 0.014 inch guidewire through the balloon catheter and crossed the stenosis of the dorsalis pedis artery again, utilizing a roadmap technique. They treated the stenosis of the dorsalis pedis artery at and below the ankle with a 2.5 mm by 20 mm CryoPlasty balloon. A post-op control angiogram showed significant improvement in the diameter of the dorsalis pedis artery with a focal area of spasm at its mid-portion. The patient tolerated the procedure well and the multidisciplinary team noted a strong, palpable dorsalis pedis pulse after the procedure.
An Early Glimpse At CryoPlasty Study Results
Preliminary findings from a prospective, multicenter trial show that CryoPlasty therapy may be beneficial for patients with critical limb ischemia. The preliminary results, which were reported by James D. Joye, DO, recently at the 17th Annual International Symposium on Endovascular Therapy, focused on 25 patients who had critical limb ischemia and an average age of 72. With an average follow-up of 45 days, researchers found that the average residual stenosis after CryoPlasty treatment (performed at 8 ATM and –10ºC) in the first 22 patients was 19.3 percent. The average baseline stenosis in these patients was 87.3 percent +/- 10.54 percent. Researchers also reported an improved distal pulse in 17 out of the first 20 patients. They noted that they could not measure pulses in the remaining three patients of the study due to a dressing on their leg.
Final Notes
Subsequently, the patient underwent a transmetatarsal amputation on the left foot on Oct. 6. This allowed for ambulation without a prosthesis. The patient experienced significant bleeding postoperatively as well as bounding pulses. The patient tolerated the procedure and anesthesia well and was discharged to an intermediate care facility for physical therapy and wound care. This case study demonstrates the suitability of delivering the small vessel cryoballoon to a distal lesion below the ankle. The patient underwent angioplasty without the creation of a prominent dissection across a 30 mm length occluded segment and two additional sites. There was vigorous bleeding during surgery, a favorable prognostic sign, and the surgical wound was healing at three weeks. While the primary objective in this case is limb salvage and wound healing, further follow up in a controlled environment will be necessary before one can make statements regarding patency rates. Dr. Aruny is an Assistant Professor and Co-Chief of Vascular and Interventional Radiology at Yale University School of Medicine. Dr. Aruny can be contacted at john.aruny@yale.edu. Dr. Blume is a Clinical Assistant Professor in the Department of Orthopaedics and Rehabilitation at the Yale University School of Medicine. He is also a Fellow of the American College of Foot and Ankle Surgeons, and is the Director of Limb Preservation at the Yale New Haven Hospital in New Haven, Conn. Dr. Sumpio is the Chief of the Section of Vascular Surgery at the Yale University School of Medicine. Dr. Buren is a Chief Resident in the Section of Podiatric Surgery within the Department of Orthopedic Surgery at the Yale University School of Medicine. Editor’s Note: This article was adapted with permission from the December 2004 issue of Vascular Disease Management.
References:
1. Spinosa DJ, Leung DA, Matsumoto AH, et. al. Percutaneous intentional extraluminal recanalization in patients with chronic critical limb ischemia. Radiology 2004; 232:499-507.
2. Dotter CT, Judkins MP. Transluminal treatment of arteriosclerotic obstruction: Description of a new technique and a preliminary report of its application. Circulation 1964;30:654-670.
3. Schwarten DE. Clinical and anatomical considerations for nonoperative therapy in tibial disease and the results of angioplasty. Circulation 1991;83(2 suppl):I86-I90.
4. Bolia A, Brennan J, Bell PR. Recanalisation of femoro-popliteal occlusion: improving success rate by subintimal recanalisation. Clin Radiol 1980;40:325.
5. Lipsitz EC, Ohki T, Veith FJ, et. al. Does subintimal angioplasty have a role in the treatment of severe lower extremity ischemia? J Vasc Surg 2003;37:386-91.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}