

ADVERTISEMENT
A Closer Look At Lateral Talonavicular Instability In Athletes




When thinking of talonavicular instability, we all tend to think of the severely collapsed flatfoot deformity. Certainly, there is a prevailing emphasis on medial subluxation in the literature. Well, instead of focusing on medial talar bulging, I’d like to offer a closer look at lateral bulging of the talar head or lateral talonavicular subluxation.
As we all know, the talonavicular joint is a ball and socket-style joint.1 The joint has capsular support medially and laterally, but very little ligamentous support structures. All the ligaments of this joint are dorsal and plantar.1 As a result, patients are susceptible to gradual attenuation of the capsule. We are all accustomed to exploring the posterior tibial tendon sheath and talonavicular capsule medially, but very few are familiar with addressing the lateral capsule.
Talonavicular instability is part of a continuum of symptoms. This is rarely the primary issue for athletes. The majority of the 150 or so cases I have evaluated and eventually treated over my career all had ankle instability for a long period of time. They all had a cavus foot type. There was not one case involving pes planus. Many patients had a slight varus tilt of their calcaneus, which was more positional than structural.
Accordingly, I haven’t had to do that many tibial osteotomies, Dwyer calcaneal osteotomies or lateral sliding calcaneal osteotomies. All the patients I saw had tighter talocalcaneal angles on weightbearing anteroposterior (AP) X-ray views. Once you examine these patients, it becomes incredibly obvious. If you think it is abnormal to see the talar head medially, to see it laterally can be downright freaky. Simply invert the foot and out comes the talar head (see the first right photo above).
Pertinent Diagnostic Insights
Symptom-wise, many of these patients will not only complain of instability but will present with burning nerve pain on top of the foot or shooting pain down to their second through fourth toes. Many times, when you examine these patients, you are able to see the intermediate dorsal cutaneous nerve. It lies lateral to the talar head and often becomes stretched with inversion. In some patients, the nerve will actually slide off the side of the talar head, creating shooting pain. The nerve actually subluxes over the curvature of the talar head with circumduction of the foot. As you run your finger over the nerve like a guitar string, the patient will experience paresthesias.
Diagnostically, we all need to start with weightbearing foot X-rays. Don’t forget to also obtain ankle films because one should also expect to see ankle instability and potential pathology. Magnetic resonance imaging (MRI) is not very valuable for evaluating the talonavicular joint. You often may see a pouch of fluid on the T2 image laterally but rarely see much else that pertains to the talonavicular joint.
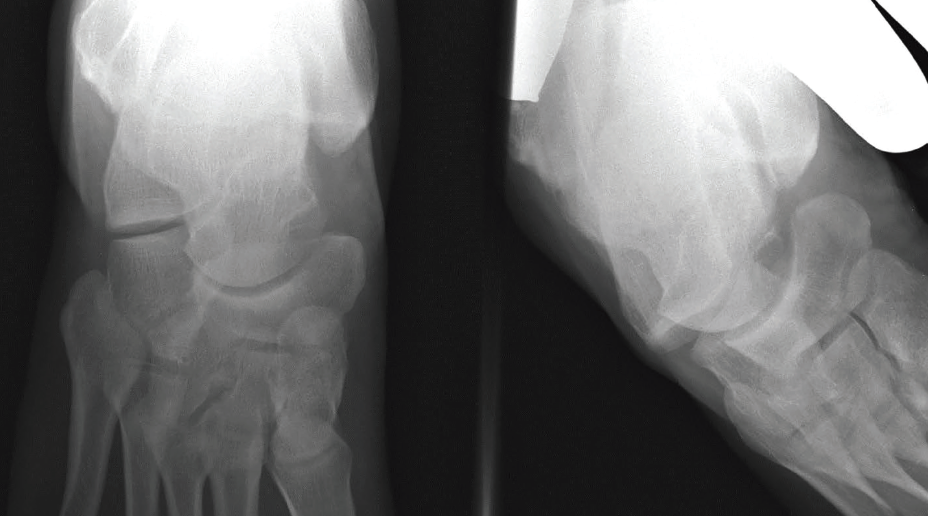
The key is performing stress X-ray examination. You need to put the foot in a neutral AP position, then invert the ankle and maintain the AP view of the foot. With stress films (see radiographic images above), you can see the talar head subluxing laterally out the talonavicular joint. Many times, you will see 50 percent subluxation of the talar head.
You can imagine why we see medial subtalar dislocations where the talar head dislocates laterally. Once that talar head gets pinned against the navicular, it is so hard to reduce in a closed fashion. I always theorized that patients with chronic instability are far more prone to medial subtalar dislocations. Accordingly, the majority of subtalar dislocations with sports I have ever seen were inversion-style injuries.
An Evolving Surgical Approach To Talonavicular Instability
Once you figure out the degree of instability, the question becomes how to stabilize it. As someone who has perfected my repair over the years, I have gone from attempting arthroscopic capsular shrinkage of the capsule via a talonavicular arthroscopy to open repairs. The literature for ankles and shoulders claims capsular shrinkage can tighten the capsule by 50 percent.2-4 However, I have never seen better than 30 percent in my experience. So if the stress exam shows 50 percent subluxation, you know right away that capsular shrinkage will not reduce the talar head.
For typical cases, I experimented with open repairs. Initially, I simply utilized a Brostrom-style pants-over-vest repair with 0-Vicryl (polyglactin 910) and a lateral capsulorraphy. This is no different than what we do every day with our bunion repairs with a vertical capsulotomy. In my military and athletic communities, I had repeated failures with just absorbable suture so I progressed to non-absorbable suture. I did notice improvements but began to see issues with suture knots after using #5 Ethibond (braided polyethylene terephthalate) for strength.
As I continued to play with all the new anchor systems, I landed on the InternalBrace® from Arthrex. The InternalBrace requires two SwiveLocks® (Arthrex), which does make it knotless. However, I found two issues with the technique. First, the FiberTape rubs on the talar head cartilage when one places it intracapsularly. When I tried to place it in an extracapsular manner, I found it painful working around the capsule itself and often fought around the soft tissue to get the SwiveLocks in place. Second, in my experience, I think the InternalBrace locks up the talonavicular joint. Biomechanically, we need talonavicular range of motion.
I finally landed on a compromise of anchors: one or two SutureTaks® (Arthrex) and one SwiveLock. I will use a SutureTak in the lateral navicular. I employ four non-absorbable sutures. Once I place the suture through the distal capsule, I subsequently reduce the talar head and secure the suture with the SwiveLock in the talar head/neck. This is probably the hardest part. You want to ensure that you do not skive dorsal or plantar in the talus, which can lead to fracture. As you drill, please be careful to ensure that you are in solid bone. Once the SwiveLock is secure, the joint is stable but not too tight to prevent some talonavicular motion. Simply bolster the capsule with some absorbable suture.
Understanding The Complications Associated With Talonavicular Stabilization
I have to admit, the majority of my patients have significant pain postoperatively. I attribute this to retracting the intermediate dorsal cutaneous nerve out of the way. Paresthesias and pain can progress to complex regional pain syndrome (CRPS) but the majority of these instances resolve with time. Many of these patients can and do require gabapentin, alcohol injections and physical therapy. Unfortunately, so many of these patients present with neurologic symptoms prior to surgery that is almost customary to expect symptoms to intensify post-surgery. Again, this is why, when feasible, I will consider an arthroscopic approach versus an open repair.
Over the past 10 years at the General Leonard Wood Army Community Hospital in Ft. Leonard Wood, Mo., I have performed 49 open repairs and one arthroscopic capsular shrinkage. All 50 cases included concomitant procedures. All 50 patients had normal to higher calcaneal inclination angles. Only one patient, who developed CRPS, failed to return to sports or full duty. All but the talonavicular arthroscopic patient developed some postoperative neuritis.
I have had my share of failures due to injuries post-surgery within the first three months. Amazingly, only one patient required revision surgery and it involved removing a backed-out SwiveLock anchor. I have performed repeat stress exams on a select few concerning cases and I did not see any subluxation over 25 percent in these cases. Many of them felt unstable to me but the patients did not complain of pain or a sense of instability. Just as we see with ankle instability, there are plenty of athletes and soldiers who have quantifiable instability but are asymptomatic. As a result, I leave the talonavicular instability alone if the stress exam yields less than 30 percent subluxation.
In some cases, once one addresses the ankle instability, there can be a reduction of talonavicular instability. As a result, I now stress the talonavicular joint first and then stress it post-Brostrom prior to opting for open repair. I suspect that I may be able to divert from an open to an arthroscopic capsular shrinkage on a few cases or simply avoid surgery altogether.
I have definitely had challenges in these patients with post-op neuritis
but I am not sure how I can avoid it. A few years ago, when I gave a lecture at the Missouri State Podiatry Meeting, someone suggested that I try going medial. The thought was if you secure the talar head, it will not rotate laterally. I did try this approach but I was not thrilled with the anchor placement nor the amount of dissection required. The medial capsule is far more robust than the lateral capsule. It seemed like I was doing more work and fighting to place the anchors around the posterior tibial tendon insertion. The patient did okay. While I avoided the nerve dissection in this case, I did not feel good about working in an area where the patient had no pain. I have not tried that approach again.
Final Thoughts
As one can see, I have spent 15 years studying this condition that I see almost exclusively in athletes and soldiers. There has been a lot of trial and error. Without significant research or even case reports to guide me, I have made my share of mistakes. I am hopeful that those of you who treat athletes will pay attention to the foot, not just the ankle. The stress exam is very impressive. There is no doubt that postoperative neuritis is and will remain a significant issue, but more often, patients present with neuritis preoperatively. I would pose that this is no different than what we all see with tarsal tunnel surgery, namely that patients who come to us with nerve pain will likely leave with nerve pain. We just hope the symptoms are better than before.
As with anything, I am getting more selective as I get older. If I have a patient who has no symptoms at the talonavicular joint, I will more often consider leaving it alone and simply address the primary area of pain and instability. I figure this does not burn any bridges and I can always go back and address the patient’s talonavicular instability in the future.
Dr. Spitalny is a staff podiatrist at the General Leonard Wood Army Community Hospital in Ft. Leonard Wood, MO, and adjunct faculty with the DePaul Podiatric Surgical Residency Program in St. Louis.
1. Haouimi A, Cheng J. Talonavicular joint. Radiopaedia. Available at: https://radiopaedia.org/ articles/talonavicular-joint?lang=us . Accessed August 31, 2020.
2. Vuerberg G, de Vries JS, Krips R, Blankevoort L, Fievez AWFM, van Dijk CN. Arthroscopic capsular shrinkage for treatment of chronic lateral ankle instability. Foot Ankle Int. 2017;38(10):1078-1084.
3. Longo UG, Rizzello G, Loppini M, et al. Multidirectional instability of the shoulder: A systematic review. Arthroscopy. 2015;31(12):2431-2443.
4. Medvecky MJ, Ong BC, Rokito AS, Sherman OH. Thermal capsular shrinkage: Basic science and clinical applications. Arthroscopy. 2001;17(6):624-635.


