

ADVERTISEMENT
Understanding The Connection Between Diabetes And Depression
When it comes to patients with diabetes, the important roles of depression and distress have received more attention in the literature within the past year.1-6 While these topics are typically off our radar screens, having a stronger understanding of these connections can enable podiatric physicians to make meaningful differences in our patients’ lives. We care for patients in transitional health states across the continuum of care when these problems are more likely to surface. We also have more frequent contacts that can make us more sensitive and responsive to subtle changes in our patients’ mental health.
It is hardly a stretch to say that treating patients with diabetes can present a large challenge. Frequently our patients have lost the important sensory feedback loop of the gift of pain.7 This is coupled with emotional, mental, familial, occupational and social challenges of adhering to a demanding treatment regimen and prescribed lifestyle changes. All of this can rapidly cascade into frustrating clinical encounters in which little progress happens from both the physician and patient perspectives.
How can the podiatric physician possibly address these issues in an effective manner during a 15-minute encounter in a busy practice?4 Fortunately, there are a couple of simple clinical pearls and important signals that can better elucidate these important clinical states in our patients.4,8,9
What The Literature Reveals About Depression
A recent meta-analysis of nine studies suggests that depressed people have a 37 percent increased risk of developing type 2 diabetes.10 Depression is twice as common in patients with diabetes.11 While a meta-analysis suggests the prevalence of depression in patients with diabetes is around 11 percent, it may be as high as 32 percent in patients with a diabetic foot ulcer (DFU).1,12 Depressed patients also have poorer adherence to diabetes treatment regimens. Depression is clinically important because it is associated with higher rates of mortality in patients with diabetes.1 Fortunately, researchers have shown that increased recognition and treatment of depression in patients with diabetes can help reduce this excess mortality.5
Unfortunately, depression often is frequently under- or undiagnosed.13 We are often very busy addressing competing clinical demands when patients frequently present in these vulnerable health states. Do we miss some subtle changes in their mental status? Does this happen when a patient is first diagnosed with diabetes? Is it possible that we are missing some telltale signs in behavior when we first diagnose a patient with neuropathy? Our knee-jerk reaction might be to inundate patients with a list of dos and don’ts for modifying foot care behaviors. Are we adding to the patient’s distress?
Do we overlook these things when treating a patient who has presented with new foot ulcers or do we miss subtle signs in a post-op visit after limb salvage surgery? This is a time when we tend to saddle our patients and their caregivers with offloading instructions, wound care regimens and a list of dangerous conditions to look out for. We have to treat the urgent clinical problem of the moment. However, we should also have a heightened awareness to detect these sometimes subtle changes in mental status.
Various cross-sectional studies have implicated poor mental health status as possibly having a role in foot complications, namely ulcer healing or amputation.14-18 Two cross-sectional studies reported that patients with diabetes-related foot ulcers had a lower health-related quality of life and functional status than diabetes controls and amputation patients.14,15
In a decision analysis model, Eckman and colleagues reported health-related quality of life using the SF-36 in the following groups of patients with diabetes: controls without history of ulcer or amputation; those with foot ulcers; and those with a history of amputation. The controls had the highest SF-36 scores in physical function and general health perception while the lowest SF-36 scores occurred among patients with a diabetic foot ulcer. Amputees scored higher than current ulcer patients.15
Carrington and colleagues observed a similar trend when they studied hospital anxiety and depression in a similar cross-section of patients. For quality of life and psychological adjustment to illness, control patients scored higher than patients with amputation. Foot ulcer patients scored lower than patients with amputation. The same study reported that patients with foot ulcers had higher levels of hospital anxiety and depression than control patients and amputees.14
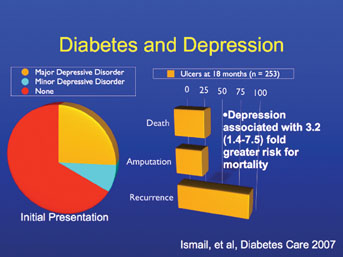
Ismail and colleagues attempted to better elucidate the role of depression in a prospective cohort study of patients with diabetes and a new foot ulcer with an ankle-brachial index (ABI) > 0.5.1,6 In following 253 patients over 18 months, the researchers observed for ulcer recurrence, amputation or death. They categorized depression as major, minor or absent via a semi-structured diagnostic interview. There was a three-fold increased risk of death in the 32 percent of patients with DFUs who had either major or minor depression. This was not fully explained by adherence as there were no associations between depression and baseline or glycemic control at the end of the study.1
Is It Distress Or Depression?
The prevalence of depression seems to be higher when researchers use patient surveys as opposed to structured interviewing techniques. Experts suggest this may represent depressive symptoms in people without clinical depression or they may represent distress.2
Researchers have measured diabetes-related distress by using the domains of emotional burden, physician-related distress, regimen-related distress and diabetes-related interpersonal distress.19 This appears to be an important clinical distinction as previous studies have shown adequate treatment of depression does not significantly change diabetes-related outcomes.2
However, general and diabetes-related distress has been associated with behavioral and biological outcomes. This could partially explain some of the findings from Ismail and colleagues that while depression was associated with mortality, it was not associated with amputation or ulcer recurrence. Other studies failed to find an association between depressive symptoms and DFUs.8 An unrecognized reservoir of patients with distress could be partially responsible for the poor adherence researchers have observed with prescribed offloading treatment regimens for DFUs.20,21 Our high-risk patients wear their prescribed shoes or offloading device only 22 to 28 percent of the time.20,22 Most of the time, this ambulation occurs within the home, a place many of our patients consider to be “safe zones” for walking without these prescribed devices.
Examining The Link Between Depression And Neuropathy
One should make a finer clinical distinction when referring to depressive symptoms in patients with diabetes-related peripheral neuropathy (DPN).8,23 As clinicians, we may use clinical thresholds, such as sleep disturbance or functional limitation, for treating painful neuropathy. Important work by Vileikyte and colleagues identified another important subgroup of patients that could benefit from our care. They created and validated a neuropathy-specific instrument known as the Neuroqol.8,23,24 The Neuroqol is a 43-item questionnaire that has three domains of pain, numbness and unsteadiness. Vileikyte and colleagues later studied 492 patients with diabetes and peripheral neuropathy. They measured neuropathy based on the Neuropathy Disability Score and vibration perception threshold (VPT). They measured symptoms of neuropathy using the Neuroqol and assessed depressive symptoms via the Hospital Anxiety and Depression Scale. Researchers associated depressive symptoms with the clinical measures of neuropathy. All three domains of the Neuroqol (pain, numbness and unsteadiness) were associated with depressive symptoms. Therefore, the association of neuropathy severity and depressive symptoms was mediated by neuropathic symptoms. Self-reported unsteadiness was highly prevalent at 23 percent and researchers demonstrated higher associations with depressive symptoms over pain and numbness.8
The other clinical significance in this important study is that there were two possible psychosocial links to the association of depressive symptoms and neuropathy symptoms. This included the actual impairment of physical functioning affecting social and family roles, and the cognitive representation of neuropathy symptoms.8
Keys To Screening In A Busy Practice And How It Can Be Beneficial
Mark Peyrot, PhD, one of the co-authors of the above described study, discussed the clinical implications of these findings in an intriguing CLEARcast interview with David Armstrong, DPM, PhD. Peyrot has also described feasible approaches to use in the aforementioned 15-minute visit window.4
First, we can ask our patients if they feel unsteady on their feet. If so, strength and balance training interventions can help people feel steadier on their feet.25,26 We can inquire about potential obstacles in their home and work environment. Ambulatory aids can also help. Bracing may be useful as well.27
Patients with diabetes frequently exhibit a conservative gait strategy, maintaining a wide base, slower speed and increased double support time. Much of their ankle torque is decreased because of this strategy. They tend to generate more of their ankle torque from passive means.27 Clinicians have been hesitant to prescribe braces that contact the skin in neuropathic patients. However, this may not be a problem in properly selected patients who can check their skin. One may also avoid this potential concern by using a non-contact brace such as the double upright brace.
Secondly, one could consider screening for depression. As previously described, it is difficult for us as podiatrists to diagnose depression. However, Peyrot suggests we can screen for this disabling condition with two simple questions:
• During the past two weeks, have you felt down, depressed or hopeless?
• Over the same time period, have you lost interest or pleasure in doing things?
Affirmative answers to either of these questions might prompt a mental health referral. We could use the above strategy to help our patients cope with anhedonia or losing pleasure in life’s activities. This may stem from functional limitation in participating in a hobby or leisurely activity. By clarifying these situations, it is possible that there are rehabilitative techniques, environmental changes, adaptive equipment, bracing or ambulatory aids that might keep our patients participating in these important activities.
The second implication for depression screening is identifying the untapped reservoir of distress. By identifying distress, it may help the podiatrist understand potential sources and modify treatment approaches if feasible. The alternative would be to refer to a certified diabetes educator in designing a behavior modification program.
We recognize the importance of self-care behaviors in our patients with diabetes. Typically, we may give a laundry list of dos and don’ts, or provide an educational pamphlet. The room for improvement with this approach is highlighted by recent work from Johnston and colleagues. They surveyed 772 veterans with high-risk foot conditions. Despite being in the VA system with ready access to certified diabetes educators and podiatrists, only 32 percent of patients reported performing daily foot inspections. Over half of them could not see or reach their feet despite foot stools and mirrors.28
A better understanding of the sources of distress will help better guide various behavioral approaches. Peyrot and Rubin recently wrote a very thoughtful review of these approaches.4 Behavioral models can target specific factors such as motivation, facilitators and inhibitors, intentions and triggers. The specific interventions then use goal setting, motivational interviewing, problem solving, coping skills training, environment change, behavioral contracting, self-monitoring, incentives and rewards, and social support.
Further exploration of these limitations will elucidate a patient’s cognition of the problem. This can be helpful in guiding a behavioral intervention. If the patient wants to change a specific behavior, it might be better to emphasize an empowerment model. If the provider decides that the behavior is important to change, it might be best to use a transtheoretical model.4 The selective use of these models in future patient education studies may better demonstrate their effectiveness.
Final Notes
With continued technological advances in communication devices and increasingly more prevalent use of these devices, there are opportunities to imbed new processes into our daily practices without adding to the provider workload.29
Your office staff could routinely ask the previously presented questions. You can leverage existing electronic medical record (EMR) platforms to incorporate touch screen kiosks in waiting rooms. These kiosks can gather this information in real-time for podiatrists to act on the data. Similar strategies can work with cell phones, PDAs and from online sources. I wonder if we sometimes overlook investing in this equipment in favor of purchasing the newest surgical treatment modality. While both are important, there is a real opportunity to identify a serious condition that can affect our patients’ five-year mortality.
Identifying depression and distress in our patients with diabetes presents an important clinical opportunity for us to make an important impact in our patients’ lives. The simple identification of gait unsteadiness will lead to important treatment opportunities. Patients are reluctant to share this disability with us because they chalk it up to aging or as being irreversible. Identification of a major depressive disorder for medical management could help mitigate the three-fold risk of death that researchers have observed in high-risk patients with diabetes. Identifying diabetes distress could help us assist our patients in overcoming counterproductive behaviors or it could help us make appropriate referrals for a more individualized strategy.
Dr. Wrobel is an Associate Professor of Medicine and Director for Outcomes Research at the Center for Lower Extremity Ambulatory Research (CLEAR) at the Dr. William M. Scholl College of Podiatric Medicine at Rosalind Franklin University of Medicine and Science. He is also a Clinical and Research Podiatrist at the Captain James A. Lovell Federal Health Care Center in North Chicago, Ill.
The author thanks David G. Armstrong, DPM, PhD, for his thoughtful review of this article.
References:
1. Ismail K, et al. A cohort study of people with diabetes and their first foot ulcer: the role of depression on mortality. Diabetes Care 30(6): 1473-9, 2007.
2. Fisher L, et al. Clinical depression versus distress among patients with type 2 diabetes: not just a question of semantics. Diabetes Care 30(3): 542-8, 2007.
3. Fisher L and Glasgow RE. A call for more effectively integrating behavioral and social science principles into comprehensive diabetes care. Diabetes Care 30(10): 2746-9, 2007.
4. Peyrot M and Rubin RR. Behavioral and psychosocial interventions in diabetes: a conceptual review. Diabetes Care 30(10): 2433-40, 2007.
5. Bogner HR, et al. Diabetes, depression, and death: a randomized controlled trial of a depression treatment program for older adults based in primary care (PROSPECT). Diabetes Care 30(12): 3005-10, 2007.
6. Winkley K, et al. Risk factors associated with adverse outcomes in a population-based prospective cohort study of people with their first diabetic foot ulcer. J Diabetes Complications 21(6): 341-9, 2007.
7. Brand PW. Tenderizing the foot. Foot Ankle Int 24(6): 457-61, 2007.
8. Vileikyte L, et al. Diabetic peripheral neuropathy and depressive symptoms: the association revisited. Diabetes Care 28(10): 2378-83, 2005.
9. Peyrot M, Armstrong DG. Unsteadiness, Uncertainty, Depression, and Amputation, in CLEARcast. 2007. p. 30 minutes.
10. Knol MJ, et al. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia 49(5): 837-45, 2006.
11. Eaton WW, et al. Depression and risk for onset of type II diabetes. A prospective population-based study. Diabetes Care 19(10): 1097-102, 1996.
12. Anderson RJ, et al. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 24(6): 1069-78, 2001.
13. Gelenberg AJ and Hopkins HS. Assessing and treating depression in primary care medicine. Am J Med 120(2): 105-8, 2007.
14. Carrington AL, et al. Psychological status of diabetic people with or without lower limb disability. Diabetes Res Clin Pract 32(1-2): 19-25, 1996.
15. Eckman MH, et al. Foot infections in diabetic patients. Decision and cost-effectiveness analyses. JAMA 273(9): 712-20, 1995.
16. Ragnarson Tennvall G and Apelqvist J. Health-related quality of life in patients with diabetes mellitus and foot ulcers. J Diabetes Complications 14(5): 235-41, 2000.
17. Nabuurs-Franssen MH, et al. Health-related quality of life of diabetic foot ulcer patients and their caregivers. Diabetologia 48(9): 1906-10, 2005.
18. Willrich A, et al. Health related quality of life, cognitive function, and depression in diabetic patients with foot ulcer or amputation. A preliminary study. Foot Ankle Int 26(2): 128-34, 2005.
19. Polonsky WH, et al. Assessment of diabetes-related distress. Diabetes Care 18(6): 754-60, 1995.
20. Armstrong DG, et al. Activity patterns of patients with diabetic foot ulceration: patients with active ulceration may not adhere to a standard pressure off-loading regimen. Diabetes Care 26(9): 2595-7, 2003.
21. Armstrong DG, et al. Continuous activity monitoring in persons at high risk for diabetes-related lower extremity amputation. J Am Podiatr Med Assoc 91: 451-455, 2001.
22. Knowles EA and Boulton AJ. Do people with diabetes wear their prescribed footwear? Diabet Med 13(12): 1064-8, 1996.
23. Vileikyte L, et al. Patient Interpretation of Neuropathy (PIN) Questionnaire: An instrument for assessment of cognitive and emotional factors associated with foot self-care. Diabetes Care 29(12): 2617-24, 2006.
24. Vileikyte L, et al. The development and validation of a neuropathy- and foot ulcer-specific quality of life instrument. Diabetes Care 26(9): 2549-55, 2003.
25. Balducci S, et al. Exercise training can modify the natural history of diabetic peripheral neuropathy. J Diabetes Complications 20(4): 216-23, 2006.
26. Richardson JK, Sandman D and Vela S. A focused exercise regimen improves clinical measures of balance in patients with peripheral neuropathy. Arch Phys Med Rehabil 82(2): 205-9, 2001.
27. Salsich GB, Brown M and Mueller MJ. Relationships between plantar flexor muscle stiffness, strength, and range of motion in subjects with diabetes-peripheral neuropathy compared to age-matched controls. J Orthop Sports Phys Ther 30(8): 473-83, 2000.
28. Johnston MV, et al. Personal and treatment factors associated with foot self-care among veterans with diabetes. J Rehabil Res Dev 43(2): 227-38, 2006.
29. Wrobel JS, et al. Diabetes-related foot care at 10 Veterans Affairs medical centers: must do's associated with successful microsystems. Jt Comm J Qual Patient Saf 32(4): 206-13, 2006.



{kind=link}
{kind=link}