

ADVERTISEMENT
Troubleshooting AFOs
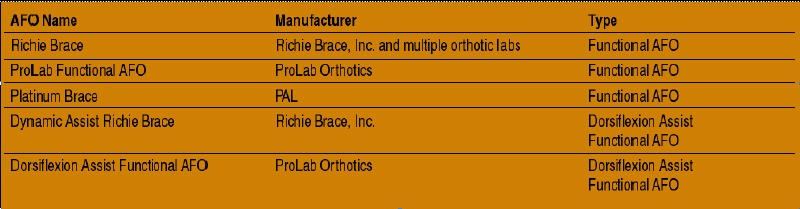
In 1996, Douglas Richie Jr., DPM, introduced the first ankle foot orthosis (AFO) to incorporate a functionally balanced foot orthosis. Podiatrists have long utilized AFOs to control ankle joint motion. However, the AFO designed by Dr. Richie was the first AFO to also provide the benefits of functional correction of the foot. These additional benefits included greater control of the subtalar joint, midtarsal joint stability and enhancement of the windlass function. The result was a rapidly accepted new modality that became a primary treatment in the podiatric profession for pathologies including adult acquired flatfoot, ankle DJD and lateral ankle instability. These “functional AFOs” are now available from many orthotic laboratories under several brand names (see “A Guide To Available Ankle Foot Orthoses” below). However, as with any DME item, patients wearing functional AFOs can develop comfort, fit or function problems. It is imperative that the prescribing physician be adept at troubleshooting any situation that may occur. With this in mind, let us take a closer look at two common complaints – medial malleolar irritation and talonavicular irritation – that patients may experience with functional AFOs.
Understanding The Potential Causes Of Malleolar Irritation
Irritation of the medial malleolus is the most common patient complaint with functional AFO therapy. There are several situations that can lead to this problem. These causes include improper hinge placement, medial displacement of the distal tibia, improper negative casting, improper positive castwork and lack of shoe stability. Improper placement of the medial hinge can lead to malleolar irritation. This is most likely to occur if the physician fails to mark the malleoli appropriately or if he or she uses an improper casting position. To avoid this problem, it is always imperative to mark the malleoli and ensure that the mark transfers to the plaster cast. If one utilizes an STS sock rather than plaster to cast the foot, then the clinician can mark the malleoli on the outside of the sock while it is still on the foot. Alternatively, one may place a piece of felt over the malleoli at the time of casting so you can capture an impression of the felt with the sock. It is also important to ensure proper casting position. If the ankle is plantarflexed during casting, one may place the hinge too far superior to the malleolus. Be sure to maintain the foot at 90 degrees to the leg during casting. If the patient has an equinus that prevents the foot from reaching 90 degrees, then the functional AFO is contraindicated.
Pertinent Pointers For Preventing Severe Medial Displacement Of The Distal Tibia
A second cause of malleolar irritation is severe medial displacement of the distal tibia during weightbearing. The medial displacement presses the medial malleolus into the medial upright, resulting in pressure and pain. To avoid malleolar irritation secondary to medial displacement, clinicians should: • perform a weightbearing examination; • plantarflex the first ray when casting; • write an anti-pronation prescription; • ensure proper positive castwork by the lab; and • recommend stable shoes. If you note a significant tibial shifting during the weightbearing examination, note it on the exam form or send a picture of the patient to the lab along with the prescription. The laboratory can adjust the medial upright to fit around the malleolus. One should plantarflex the first ray while casting in order to remove forefoot supinatus (forefoot varus due to soft tissue contracture of dorsal ligamentous structures). If clinicians do not plantarflex the first ray during the casting process, the negative cast and the subsequent orthosis will not offer adequate arch control. Inadequate arch control will allow the arch of the foot to collapse into the orthosis. This can lead to eversion of the heel with subsequent medial displacement of the medial malleolus. Prescribe anti-pronation control measures such as a minimum cast fill, medial heel skive, medial flange and deep heel cup in the foot orthosis portion of the AFO. Such a device will apply increased force medial to the axis of the subtalar joint and help prevent the patient from pronating into the medial upright. The practitioner must closely evaluate the device before dispensing it to the patient. Several laboratory errors can lead to excessive pronation and subsequent medial malleolar irritation. For example, one may notice overfill of the medial arch. If the lab adds excessive arch fill to the positive cast, the resulting orthosis will have an arch that gaps from the foot. This will allow the foot to pronate into the arch. As the foot pronates, eversion of the heel and medial motion of the medial malleolus is more likely. Another potential laboratory error is making the device too narrow. If the orthosis is too narrow, it will provide less control of excessive pronation. Clinicians may also notice incomplete balancing of the forefoot. If the laboratory does not completely balance any forefoot valgus found in the negative cast, the cast and the orthosis will retain excessive forefoot varus. Excessive varus results in a lower arch and greater potential for subtalar joint pronation and subsequent medial malleolar displacement. One should also ensure that these patients are wearing stable shoes with a firm heel counter, firm medial midsole and torsional stability. Orthotic laboratories that manufacture functional AFOs should provide lists of recommended shoes to dispense to patients.
How To Address Medial Malleolar Irritation When It Does Occur
Paying close attention to the aforementioned items will help prevent medial malleolar irritation from occurring. However, if one has dispensed an AFO to a patient and the patient subsequently presents with medial malleolar pain due to medial displacement of the medial malleolus, taking the following measures will usually correct the problem. • Modify the AFO. A simple in-office modification allows the practitioner to reshape the upright and bend it away from the prominent malleolus. Using a heat gun, focus heat on the segment just below the medial ankle pivot. When the plastic becomes pliable, push the medial limb upright downward in a slightly medial direction. This is easier to perform with two people. Have an assistant stabilize the AFO in an upright position while aiming the heat gun and push the limb upright down. Hold the position for one minute. Proceed to have the patient wear the AFO and check for adequate bending of the medial hinge. If irritation is still present, repeat these steps as necessary. • Increase pronation control. By increasing pronation control and decreasing calcaneal eversion, the medial malleolus is less likely to deviate medially. If the control features that one initially prescribes do not offer adequate control, clinicians can add simple modifications to the AFO. One of the most effective is to add a “medial heel pad.” The medial heel pad is simply a medial heel skive that you can add – via a material such as Korex or EVA – to a finished orthosis. One can test the effectiveness of this modification in the office by using 1/8-in. adhesive felt to add a varus wedge on the interior of the heel cup. If necessary, add additional layers of felt until the patient’s pain is relieved or to the point where he or she does not tolerate additional layers of felt. If this modification reduces the symptoms, return the AFO to the lab so it can add a soft medial skive to the AFO. • Prescribe shoe modifications. Even with extensive pronation control in the AFO, the patient with severe flatfoot may continue to pronate into the medial upright of the AFO. In this situation, shoe modifications that act to decrease pronation offer additional control and reduced symptoms. The most common anti-pronation shoe modifications are a medial buttress and a medial flare. • Recommend better socks. Patients wearing AFOs should avoid cotton socks. Acrylic socks such as Thor-Lo™ provide more cushion and decreased friction relative to cotton socks.
How To Prevent Talonavicular Irritation
The cause of talonavicular irritation is usually a failure to capture the weightbearing prominence of talonavicular (TN) subluxation. In this situation, a prominent TN joint is irritated by the orthotic plate as the medial flange, usually prescribed on devices for tibialis posterior dysfunction, wraps around the medial arch of the foot. In addition, as the foot pronates, the prominent navicular will be forced into the orthotic plate and lead to increased irritation. In regard to preventing talonavicular irritation, one can employ the same aforementioned techniques discussed for preventing medial malleolus irritation. In addition, in the presence of a TN prominence, the practitioner should prescribe a “sweet spot.” This sweet spot is a vacuum-formed pocket that is incorporated into the orthosis in order to accommodate the TN prominence. The orthotic laboratory should fill the sweet spot with a cushioning material such as Poron®. To guide the laboratory in proper placement of the sweet spot, mark the prominence with lipstick so it transfers to the plaster negative cast. If you are using an STS sock, place a piece of felt over the prominence at the time of casting so the sock captures an impression of the felt.
Inside Insights For Addressing Talonavicular Irritation
When one has prescribed an AFO to a patient and he or she subsequently complains of pain due to irritation of a prominent TN joint, clinicians can take the following steps. • Increase orthosis pronation control, increase shoe pronation control and prescribe acrylic socks as described above for malleolar irritation. • Have the orthotic laboratory add a sweet spot. This is a difficult adjustment to do in the office but the orthotic laboratory should be able to easily add the sweet spot by spot heating the polypropylene. To ensure proper placement of the sweet spot, mark the prominent area of the patient’s foot with lipstick and hold the orthosis against the patient's foot. The lipstick will transfer to the orthosis. Outline this lipstick with a Sharpie® pen to make the mark permanent. • Add a horseshoe pad to the orthosis to offload the prominence. This modification is particularly easy to perform if one prescribes topcovers to be “glued heel only.” This enables either the physician or the lab to add the accommodation without having to replace the topcover.
Key Principles In Prescribing Functional AFOs
In order to achieve the best clinical outcomes and prevent the problems discussed in this article, practitioners must ensure appropriate patient selection, casting technique and prescription writing. The first rule for achieving optimum clinical outcomes is to choose the correct patient for the therapy and avoid prescribing AFOs for patients who have conditions that would be contraindicated for the functional AFO. One can appropriately prescribe functional AFOs for patients with the following pathologies: posterior tibial tendon dysfunction, severe flatfoot, arthritis of the ankle/foot, ankle sprains/instability, tendonitis and/or dropfoot. Regardless of the pathology, some patients are not candidates for functional AFOs. These patients include: • those who have equinus as a primary deformity in Achilles tendonitis; • patients who have posterior group spasticity; • those who have severe subtalar joint subluxation (i.e., late Stage 3 or Stage 4); • people who weigh over 250 lbs.; and/or • people who are taller than 6'2”. Keep in mind patients who are not candidates for functional AFOs may be candidates for other types of AFOs such as a gauntlet AFO. Correct casting technique is critical to achieve optimum clinical outcomes. Correct casting includes maintaining the foot at 90 degrees to the leg with the subtalar joint in neutral position, the midtarsal joint locked and the first ray plantarflexed.
Final Notes
Just as the physician performing surgery must have the knowledge and skill to prevent most complications and treat them when they do occur, clinicians who prescribe AFOs must also have expertise in preventing and treating AFO-related complications. AFO therapy is becoming an increasingly common modality in the podiatric practice. The practitioner who has the skill to prevent and troubleshoot complications will be better able to offer his or her patients optimum clinical outcomes. Dr. Huppin is an Adjunct Associate Professor in the Department of Applied Biomechanics at the California School of Podiatric Medicine at Samuel Merritt College. He is also the Medical Director for ProLab Orthotics/USA.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}